In a previous article, Fat Grafting in Breast Reconstruction: A Major Innovation That Can Lead to Great Results, I reviewed some of the most important innovations in breast reconstruction over the last 25 years with the most recent one being the usage of fat grafting for improvement in contouring. This technique, now commonly used, has provided the means to obtain significantly improved breast reconstruction results in many situations that previously had no practical solution.
Fat grafting, however, isn’t the only relatively new major addition to the plastic surgeon’s breast reconstruction armamentarium that facilitates the potential for aesthetically superior reconstructive results. Probably of even greater importance in the advancement of breast reconstruction has been the introduction and widespread usage of acellular dermal matrices (ADM’s) such as Alloderm® and Strattice® , which are processed, non-cellular and non-antigenic tissue. These products have been somewhat revolutionary for both immediate and delayed breast reconstruction as well for revisions of previously performed breast reconstructions. Among some of their advantages have been to provide for greater predictability and control of implant position, a lowered risk for hardness developing following implant placement (known as capsular contracture) which is a particularly high risk for those who have had radiation treatments for their breast cancer, and even for thickening of very thin tissues which allows for greater support and shaping as well as a reduced risk or extent of rippling or contour irregularities.
With regard to breast implants, there are greater choices related to configuration which were not available twenty or even ten years ago. We now have what are known as high and ultra-high profile silicone breast implants which means that they provide not only greater projection but also do so with less width. In the past, the more limited breast implant choices precluded the ability to obtain more appropriate projection in many women undergoing breast reconstruction.
The following case of mine illustrates all three of these innovations and the effects that can be obtained in breast reconstruction when properly and precisely employed.
This is a 52 year old woman who underwent a right mastectomy and reconstruction elsewhere 12 years previously. This was followed five years later by a revision. On the left breast, she had undergone either a breast lift or reduction in order to obtain closer symmetry between the two sides. She saw me in consultation because she wasn’t satisfied with her results which were problematic both when wearing and when not wearing clothes. No method of padding or using inserts in her bra could camouflage the significant differences between the two sides.

A) Before right breast reconstruction revision and left mastopexy – frontal view

B) After revision of right breast reconstruction and left breast lift – frontal view

C) Before right breast reconstruction revision and left mastopexy – oblique view

D) After revision of right breast reconstruction and left breast lift – oblique view

E) Before right breast reconstruction revision and left mastopexy – side view
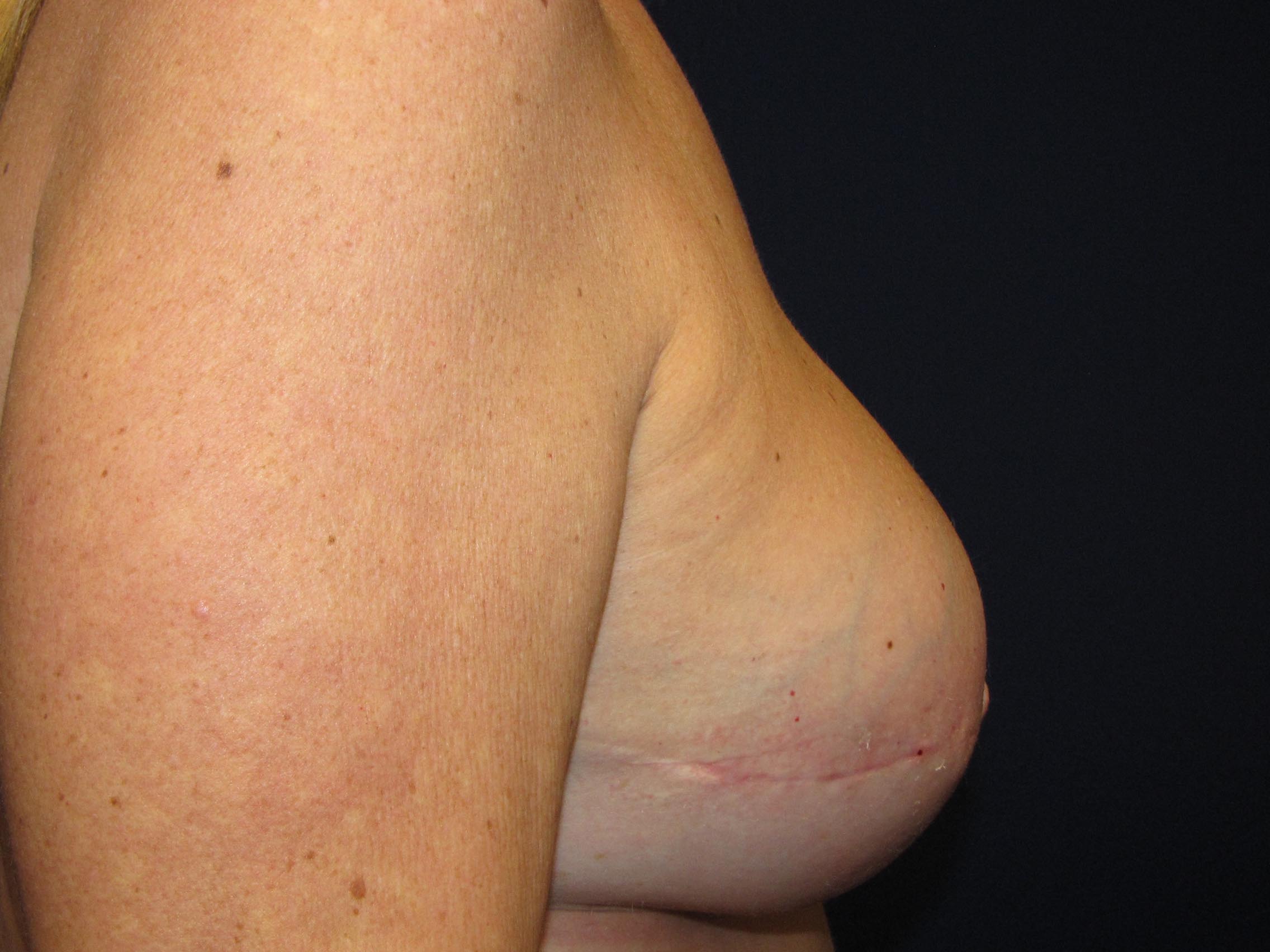
F) After revision of right breast reconstruction and left breast lift – side view
As you can see from her photos, there are multiple significant deficiencies including of contour, size and projection as well as substantial asymmetries between the two sides (Fig A, C and E). Her skin on the right was so thin that the underling saline implant could be easily felt. Furthermore, the breast was also quite firm.
How did I address all these issues?
On her right side, I released the deforming, tight scar tissue. Alloderm® was placed for shape, tissue thickening and support. Her saline implant was replaced with a much larger and a very high profile silicone breast implant. Fat injections were then employed to correct the significant contour deficiencies as well to improve the overall shape and projection. For the left side, a mastopexy was performed to better match the shape and projection of the right (Fig B, D and F).
Needless to say, she was extremely happy with her results and no longer has to wear padding in her bra.
If you would like more information on breast reconstruction including the use of fat injections or acellular dermal matrices such as Alloderm® or Strattice® or for any other plastic surgery procedure that I perform, please call my office at 480-451-3000. You can also schedule a consultation at that time.
Steven H. Turkeltaub, M.D. P.C.
Scottsdale and Phoenix, Arizona